
3 theories: Tinnitus and disorders of the temporo-mandibular joint (TMJ) and neck
https://tinnitus.org.uk/understanding-tinnitus/living-with-tinnitus/tinnitus-and-tmj/
“There are three main theories behind why problems with the TMJ may cause tinnitus, or make it worse.
- Firstly, the chewing muscles are near to others that insert into the middle ear. If they are not functioning as they should, this may have an effect on hearing and trigger tinnitus.
- Secondly, there can be a direct connection between the ligaments that attach to the jaw and one of the hearing bones that sits in the middle ear. If this ligament becomes overstrained, sprained or inflamed it can impact on tinnitus.
- Thirdly, the nerve supply from the TMJ has been shown to have connections with the parts of the brain that are involved with both hearing and the interpretation of sound.
-> Whatever the cause, the general discomfort associated with TMJ problems can also aggravate any pre-existing tinnitus.
How can TMJ problems be diagnosed?
Your dentist can often diagnose TMJ problems during an examination. If necessary, your dentist will refer you for further tests.
Disorders of the TMJ may be investigated using Magnetic Resonance Imaging (MRI) scans and sometimes by arthroscopy, a small procedure where a tiny camera is inserted into the joint.
The TMJ is connected to the ear in several ways
https://mskneurology.com/association-tinnitus-neck-tmj/
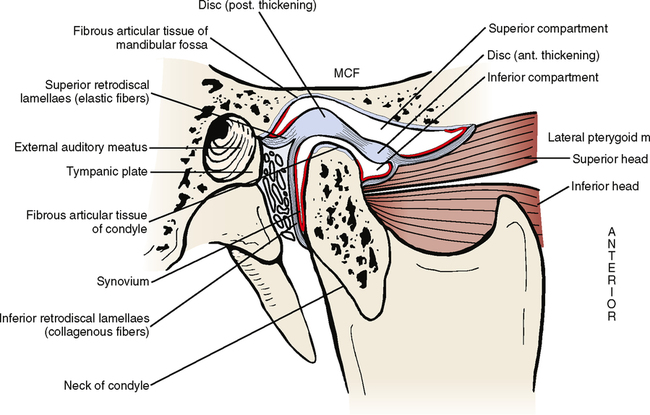
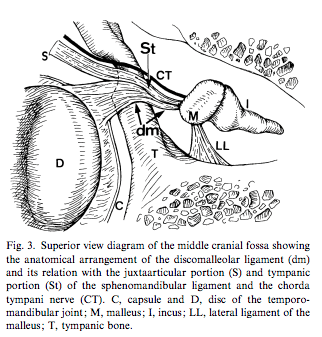
“Firstly, the superior head of the lateral pterygoid muscle may in some people be directly attached to the ossicles (the malleus / hammer) via the retrodiscal tissue and discomalleolar ligament, which is also known as Pinto’s ligament. In adults, it has been shown be to variably present in cadavers, and currently there is currently no consensus with regards to how common its attachment to the malleus really is. Some relevant studies are cited below. Either way, this shows that there is a definitely possibility of direct manipulation of the malleus via the mandible, in certain predisposed people.
Moreover; between the mandibular cavity (i.e glenoid fossa) and the mandibular condyle, lies the auriculotemporal nerve, which is a branch of the trigeminal nerve. Several studies have noted the relationship between TMD and trigeminal nerve dysfunction, and some have also noted the specific mechanism of why this occurs. Because the trigeminal nerve greatly contributes to innervation of both the external and middle ear, its impairment can and often will lead to aural symptoms, such as tinnitus, hyperacusis, and even hearing loss.
Temporomandibular joint disorder is caused by an overly retracted position of the mandibular condyle (usually due to improper growth of the maxilla and/or open mouth postures), which in turn cause shearing forces to occur within the TMJ. Between the condyle and the joint socket lies an articular disc, which helps the condyle slide through the joint spaces easily. When the condyle is resting too far back, and/or being retracted as the mouth opens (it should protract), this will once again impose compressive forces on the disc and its retrodiscal tissue, causing it to deteriorate. Ultimately, the retrodiscal tissue that holds the disc in place may partially or fully rupture, causing anterior disc displacement. When the disc displaces anteriorly, this will allow the mandibular condyle to translate even further back into the joint socket, and in many circumstances lead to compression of the auriculotemporal nerve, along with the perhaps more conspicuous TMJ pain symptoms that occur. Auriculotemporal nerve compression may also occur without discous displacement, but it is much, much rare, seeing as its compression and disc displacement have the same cause.
The auriculotemporal nerve branch, as we have discussed briefly, innervates parts of the tympanic membrane as well as parts of the external ear. Its compression may cause symptoms of pain and/or dysautonomia to spread through the nervous network in which it is connected, to variable extent (Stack & Sims, 2007). The trigeminal nerve also innervates the tensor veli palatini (which opens the eustachian tube), the tensor tympani muscle, and endolymphatic sac. The eustachian tube’s mucosa is innervated by the pterygopalatine ganglion, which also connects directly with the mandibular (trigeminal) nerve. It also connects to the tympanic plexus, which control the middle ear.
Thus, impaired signalling through these nervous pathways may alter the position of the ossicles (via the tensor tympani and stapedius muscles), endolymphatic regulation (via the endolymphatic sac), pressure regulation of the tympanic cavity, and thus also tension and mobility of the tympanic membrane. Based on this information, one may start to understand why so many tinnitus sufferers feel that their jaw is an important piece of the puzzle!
TMD may, of course, also be responsible for a whole lot of other symptoms, which are outside the scope of this article. Read my TMD article which is linked at the end of this section.”
Can you get a hernia in your ear?
https://casereports.bmj.com/content/14/5/e241839
“Herniation of the tympanic membrane is a rare benign malformation of the tympanic membrane into the external auditory canal. It may be asymptomatic or associated with symptoms such as aural fullness, tinnitus, otalgia or hearing loss.”
Otoscopy and imaging features of spontaneous temporomandibular joint herniation into the external auditory canal
https://www.birpublications.org/doi/10.1259/bjro.20200005
“STMJHs ((Spontaneous TemporoMandibular Joint(TMJ) herniation (STMJH)) have unique otoscopic, CT and MRI features. The examination strategy recommended is dynamic otoscopy and conventional CT, MRI can be chosen when the herniation is complicated by infection or otitis externa or when the patient has TMJ dysfunction; conservative management and follow-up observations are the main treatment strategy recommended.”
The foramen of Huschke
What are the symptoms of the foramen of Huschke? The symptoms of FH include conductive hearing loss, otalgia, otorrhea, and clicking tinnitus; although it may be asymptomatic [5,6,7]. Preoperative detection of the foramen of Huschke is of high importance for clinicians, especially those who perform ear and TMJ surgery for patient suffer TMJ disorders.
Persistent foramen of Huschke: clinical manifestations and complications, systematic review
https://www.sciencedirect.com/science/article/abs/pii/S2468785523000770
“Persistent foramen of Huschke should be suspected in the presence of otitis, otorrhea and masticatory tinnitus. Knowledge of this anatomical variation could help to treat certain pathology like TMJ disorders or TMJ septic arthritis.”