
Swedish (not yet completely quite ready below english texts
(NB working draft)
See also sub pages
(Below dysfunction can be partly hereditary? My mother and grandmother (as I) at older age, had a difficulty expressing themselves clearly, but probably because of their special and severe suffering, it may be what I call dysfunctional ”OlivoCochlear (Middle Pons) efferent control of in the ”Ear” Cochlea (Outer and Inner Hair Cells) Loop” – more work needed to investigate this. Among symptoms hard alarm sound clusters, where the volume control in Pons had probably a dysfunction – locked at high high level of sound). A second symtom – balance problems/dizziness – may relate also to cranial nerve VIII.
Yes, it is possible!
Very brief overvire with pictures
https://en.wikipedia.org/wiki/Olivocochlear_system
” The olivocochlear system is a component of the auditory system involved with the descending control of the cochlea. Its nerve fibres, the olivocochlear bundle (OCB), form part of the vestibulocochlear nerve (VIIIth cranial nerve, also known as the auditory-vestibular nerve), and project from the superior olivary complex in the brainstem (pons) to the cochlea.[1]”
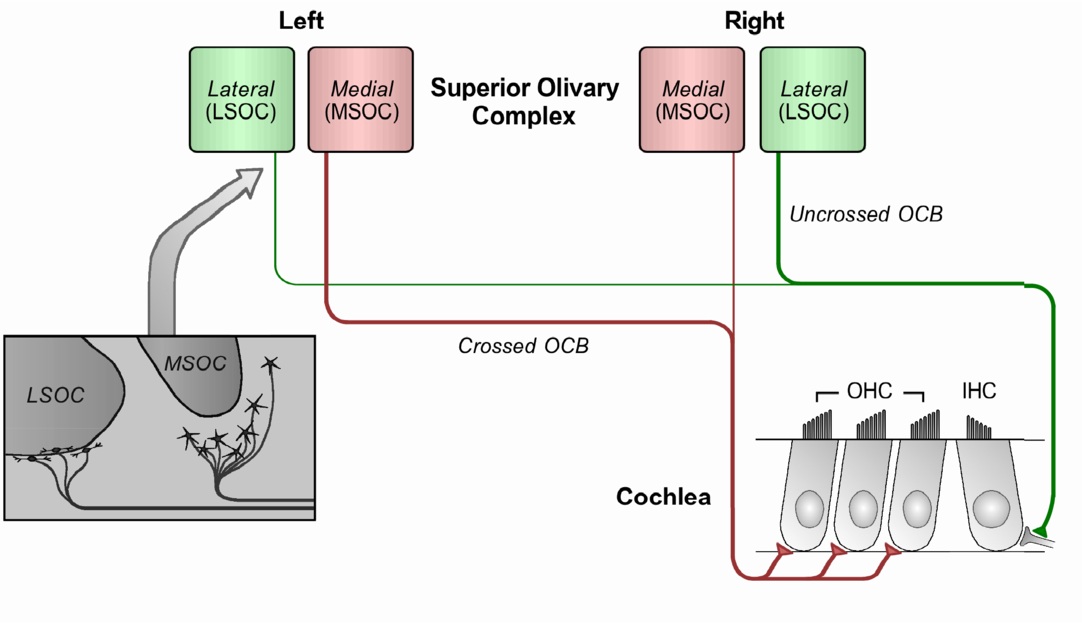
“The mammalian olivocochlear bundle, divided into medial (red) and lateral (green) systems. Both contain crossed and uncrossed fibres. The predominant fibres are represented by a thicker line. The insert (far left) shows the position of the cell bodies of the MOCS and LOCS relative to the MSOC and LSOC respectively, as observed in mammals.
“The mammalian olivocochlear bundle, divided into medial (red) and lateral (green) systems. Both contain crossed and uncrossed fibres. The predominant fibres are represented by a thicker line. The insert (far left) shows the position of the cell bodies of the MOCS and LOCS relative to the MSOC and LSOC respectively, as observed in mammals”.
The olivocochlear system is a component of the auditory system involved with the descending control of the cochlea”
Latest first
Brief: ”The olivocochlear (OC) efferent are part of brainstem-to-cochlea reflex pathways that allow stimulus-related control of the cochlea, and provide a way for the central nervous system to affect hearing at the most peripheral neural level”
Abstract: ”The anatomy and physiology of olivocochlear (OC) efferents are reviewed. To help interpret these, recent advances in cochlear mechanics are also reviewed. Lateral OC (LOC) efferents innervate primary auditory-nerve (AN) fiber dendrites. The most important LOC function may be to reduce auditory neuropathy. Medial OC (MOC) efferents innervate the outer hair cells (OHCs) and act to turn down the gain of cochlear amplification. Cochlear amplification had been thought to act only through basilar membrane (BM) motion, but recent reports show that motion near the reticular lamina (RL) is amplified more than BM motion, and that RL-motion amplification extends to several octaves below the local characteristic frequency. Data on efferent effects on AN-fiber responses, otoacoustic emissions (OAEs) and human psychophysics are reviewed and reinterpreted in the light of the new cochlear-mechanical data. The possible origin of OAEs in RL motion is considered. MOC-effect measuring methods and MOC-induced changes in human responses are also reviewed, including that ipsilateral and contralateral sound can produce MOC effects with different patterns across frequency. MOC efferent help to reduce damage due to acoustic trauma. Many, but not all, reports show that subjects with stronger contralaterally-evoked MOC effects have better ability to detect signals (e.g. speech) in noise, and that MOC effects can be modulated by attention.”
Olivocochlear Efferents: Their action, effects, measurement and uses, and the impact of the new conception of cochlear mechanical responses – PMC https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5911200/
and/or generally dysfunctions in ´”Pons: The middle portion of your brainstem that coordinates face and eye movements, facial sensations, hearing and balance.
https://my.clevelandclinic.org/health/body/21598-brainstem
See also: The role of the medial olivocochlear reflex in psychophysical masking and intensity resolution in humans: a review https://pmc.ncbi.nlm.nih.gov/articles/PMC8285664/
Summarizing: If so, then Medial Olivocochlear (MOC) complex in Pons get feedback from cochlea activities (functional or different degree of dysfunctionality) and from that control actions of cochlea probably partly via outer hair cells and its influence on inner hair cells activities (functional or different degree of dysfunctionality. If then, e.g. head trauma influence MOC then sound distortion may relate to this. In my case I have 70 years of manageable noise damage associated tinnitus suddenly become a not manageable hard permanent alarm at the same frequency as the ”old, more common tinnitus”
On other (adding?) explanation for my dysfunction may be ”sclerosing processes”, while during short sleeping periods (1-2 h) the symptoms increase perhaps due to tissue hardening ”Peripheral pons lesion location is a good discriminator of MS from vascular lesions.” https://pubmed.ncbi.nlm.nih.gov/32757905/
I have had sclerosing Basaliom Glas typ III 2017 and 2018 Prostate cancer Gleason 9 (now well treated in Helsingfors) except since 5 year MRI documented spinal dysfunction (spondylosis and foraminal spinal stenos C3-C7, L4-L5 and S1)
Working text/draft below
Pictures below from https://link.springer.com/referenceworkentry/10.1007/978-1-4614-7320-6_431-1
Anatomy of Olivocochlear Efferents
Olivocochlear efferent fibers originate in the left and right superior olivary complexes (SOCs), project to the cochlea through the vestibular nerve, enter the basal turn of the cochlea along with auditory nerve afferent fibers, and terminate in the organ of Corti. They were first described by Rasmussen (9), who originally classified them into crossed and uncrossed types, depending on whether they originated in the contralateral or the ipsilateral SOC, respectively. At present, efferents are classified into medial and lateral based upon the location of their parent cells bodies in the SOC and their site of termination (10, 11). Medial-olivocochlear (MOC) efferents originate in the medial superior olivary nuclei and terminate directly upon outer hair cells (OHCs), while lateral olivocochlear (LOC) efferents originate in the lateral superior olivary nuclei and terminate on the dendrites of type I auditory nerve afferent fibers, beneath inner hair cells (IHCs) (Figure 1).
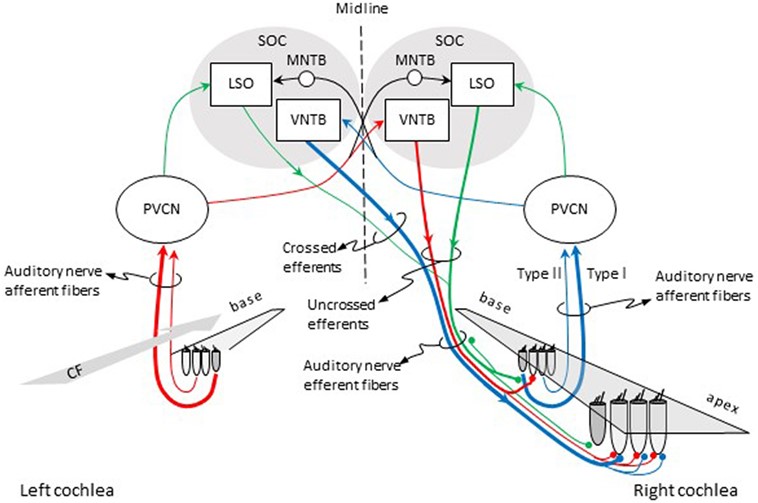
”Figure 1. Pathways for activation of medial (MOC) and lateral olivocochlear (LOC) efferent fibers to the right cochlea. Red and blue lines illustrate the pathways for activation of the contralateral and ipsilateral MOC reflexes, respectively. Green lines illustrate the pathways for activation of the LOC reflex. The thickness of each line roughly illustrates the density of innervation. Abbreviations: LSO, lateral superior olive; MNTB, medial nucleus of the trapezoid body; PVCN, postero-ventral cochlear nucleus; SOC, superior olivary complex; VNTB, ventral nucleus of the trapezoid body; CF, characteristic frequency.
Role of the medial olivocochlear efferent auditory system in speech perception in noise: a systematic review and meta-analyses
https://www.tandfonline.com/doi/full/10.1080/14992027.2023.2260951
Picture from above https://images.app.goo.gl/9vXep2zno433LQyR6
Below from The Olivocochlear System https://www.sciencedirect.com/topics/medicine-and-dentistry/olivocochlear-system
”It has been known for more than 50 years that the olivocochlear bundle (Figs. 2, 29 and 32) provides the organ of Corti with efferent innervation (Rasmussen, 1946, 1953). It should be noted that the auditory-vestibular system appears unique among sensory systems because hair cell receptors receive direct projections from the brain (Robertson, 2009). Two systems of olivocochlear neurons are recognized, the medial (MOC) and lateral (LOC) systems (Figs. 29 and 32; White and Warr, 1983; Warr et al., 1986, 1997; Spangler and Warr, 1991; Warr, 1992; Vetter et al., 1991; Vetter and Mugnaini, 1992; Cantos et al., 2000). As their names imply, their respective cell bodies are located in medial and lateral regions of the SOC.
The MOC neurons innervate the OHCs (Figs. 2, 29 and 32). About 55% of them originate on the contralateral side and the reminder on the ipsilateral side (rat: Robertson et al., 1989; Horváth et al., 2000). The projection is made up of thick myelinated axons that terminate directly on the OHCs (White and Warr, 1983; Warr et al., 1997; Horváth et al., 2000). MOC neurons (Fig. 32) generally have large cell bodies that are stellate- or triangular-shaped, and they possess tapering dendritic arbors that radiate and branch profusely (Osen et al., 1984; Vetter and Mugnaini, 1992).
More text at https://www.sciencedirect.com/topics/medicine-and-dentistry/olivocochlear-system
Olivocochlear efferent effects on perception and behavior
https://www.sciencedirect.com/science/article/abs/pii/S0378595521000411
“The role of the mammalian auditory olivocochlear efferent system in hearing has long been the subject of debate. Its ability to protect against damaging noise exposure is clear, but whether or not this is the primary function of a system that evolved in the absence of industrial noise remains controversial. Here we review the behavioral consequences of olivocochlear activation and diminished olivocochlear function. Attempts to demonstrate a role for hearing in noise have yielded conflicting results in both animal and human studies. A role in selective attention to sounds in the presence of distractors, or attention to visual stimuli in the presence of competing auditory stimuli, has been established in animal models, but again behavioral studies in humans remain equivocal. Auditory processing deficits occur in models of congenital olivocochlear dysfunction, but these deficits likely reflect abnormal central auditory development rather than direct effects of olivocochlear feedback. Additional proposed roles in age-related hearing loss, tinnitus, hyperacusis, and binaural or spatial hearing, are intriguing, but require additional study. These behavioral studies almost exclusively focus on medial olivocochlear effects, and many relied on lesioning techniques that can have unspecific effects. The consequences of lateral olivocochlear and of corticofugal pathway activation for perception remain unknown. As new tools for targeted manipulation of olivocochlear neurons emerge, there is potential for a transformation of our understanding of the role of the olivocochlear system in behavior across species”. https://www.sciencedirect.com/topics/medicine-and-dentistry/outer-hair-cell
“efferent control by Medial Olivocochlea (MOC) …
Efferent neurons control hearing sensitivity and protect hearing from noise through the regulation of gap junctions between cochlear supporting cells
https://journals.physiology.org/doi/full/10.1152/jn.00468.2021
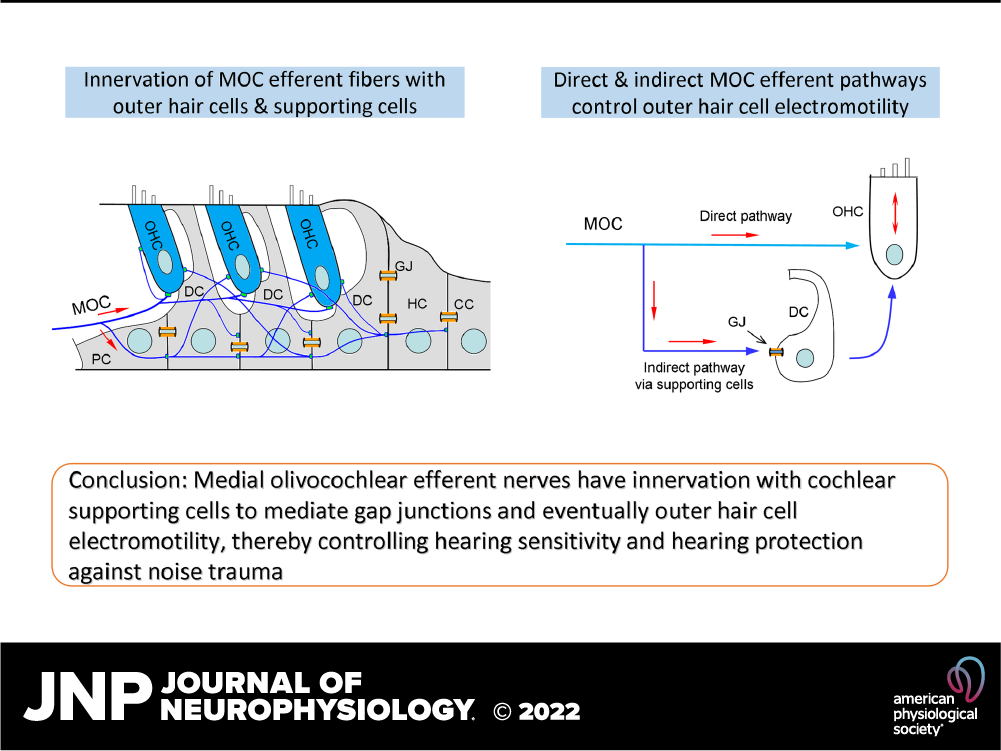
NB above conclusion: Medial olivocochlear efferent nerves have innervation with cochlear supporting gap junctions and eventually hair cell electromotility, thereby controlling hearing sensitivity and hearing portection against noise trauma outer trauma
“It is critical for hearing that the descending cochlear efferent system provides a negative feedback to hair cells to regulate hearing sensitivity and protect hearing from noise. The medial olivocochlear (MOC) efferent nerves project to outer hair cells (OHCs) to regulate OHC electromotility, which is an active cochlear amplifier and can increase hearing sensitivity. Here, we report that the MOC efferent nerves also could innervate supporting cells (SCs) in the vicinity of OHCs to regulate hearing sensitivity. MOC nerve fibers are cholinergic, and acetylcholine (ACh) is a primary neurotransmitter. Immunofluorescent staining showed that MOC nerve endings, presynaptic vesicular acetylcholine transporters (VAChTs), and postsynaptic ACh receptors were visible at SCs and in the SC area. Application of ACh in SCs could evoke a typical inward current and reduce gap junctions (GJs) between them, which consequently enhanced the direct effect of ACh on OHCs to shift but not eliminate OHC electromotility. This indirect, GJ-mediated inhibition had a long-lasting influence. In vivo experiments further demonstrated that deficiency of this GJ-mediated efferent pathway decreased the regulation of active cochlear amplification and compromised the protection against noise. In particular, distortion product otoacoustic emission (DPOAE) showed a delayed reduction after noise exposure. Our findings reveal a new pathway for the MOC efferent system via innervating SCs to control active cochlear amplification and hearing sensitivity. These data also suggest that this SC GJ-mediated efferent pathway may play a critical role in long-term efferent inhibition and is required for protection of hearing from noise trauma.
NEW & NOTEWORTHY The cochlear efferent system provides a negative feedback to control hair cell activity and hearing sensitivity and plays a critical role in noise protection. We reveal a new efferent control pathway in which medial olivocochlear efferent fibers have innervations with cochlear supporting cells to control their gap junctions, therefore regulating outer hair cell electromotility and hearing sensitivity. This supporting cell gap junction-mediated efferent control pathway is required for the protection of hearing from noise.“
https://en.wikipedia.org/wiki/Olivocochlear_system that has efferent control of and afferent feedback from the Cochlea, above all of external hair cells that ”control” the inner ones, where I have been damaged since 70 years – see audiogram (a hypothesis diagnosis proposal for my ”5 year permanent difficult to stand ”alarm left side of my head”, except 2-3 minutes during the MRI scan (while right side heard the typical MRI sound (not very nice to hear) – very hopeful)”
The olivocochlear system is a component of the auditory system involved with the descending control of the cochlea. Its nerve fibres, the olivocochlear bundle (OCB), form part of the vestibulocochlear nerve (VIIIth cranial nerve, also known as the auditory-vestibular nerve), and project from the superior olivary complex in the brainstem (pons) to the cochlea. https://en.wikipedia.org/wiki/Olivocochlear_system
Acoustically evoked responses of the MOCS (medial olivocochlear system)
https://en.wikipedia.org/wiki/Olivocochlear_system
[Electrical stimulation in the brainstem can result in (i) the entire MOCS being stimulated, (ii) a discharge rate (up to 400 s-1) much higher than is normally evoked by sound (up to 60 s-1), and (iii) electrical stimulation of neurons other than MOCS fibres. Therefore, electrical stimulation of the MOCS may not give an accurate indication of its biological function, nor the natural magnitude of its effect.
The MOCS’ response to sound is mediated through the MOC acoustic reflex pathway (see inset), which had been previously investigated using anterograde and retrograde labelling techniques (Aschoff et al., 1988; Robertson and Winter, 1988). Acoustic stimulation of the inner hair cells sends a neural signal to the posteroventral cochlear nucleus (PVCN), and the axons of the neurons from the PVCN cross the brainstem to innervate the contralateral MOC neurons. In most mammals, the MOC neurons predominantly project to the contralateral side (forming the ipsilateral reflex), with the remainder projecting to the ipsilateral side (forming the contralateral reflex).
The strength of the reflex is weakest for pure tones, and becomes stronger as the bandwidth of the sound is increased (Berlin et al., 1993), hence the maximum MOCS response is observed for broadband noise (Guinan et al., 2003). Researchers have measured the effects of stimulating the MOCS with sound. In cats, Liberman (1989) showed that contralateral sound (resulting in MOCS stimulation) reduced the N1 potential, a suppression which was eliminated upon transection of the olivocochlear bundle (OCB). In humans, the largest amount of evidence for the action of efferents has come from the suppression of otoacoustic emissions (OAEs) following acoustic stimulation.
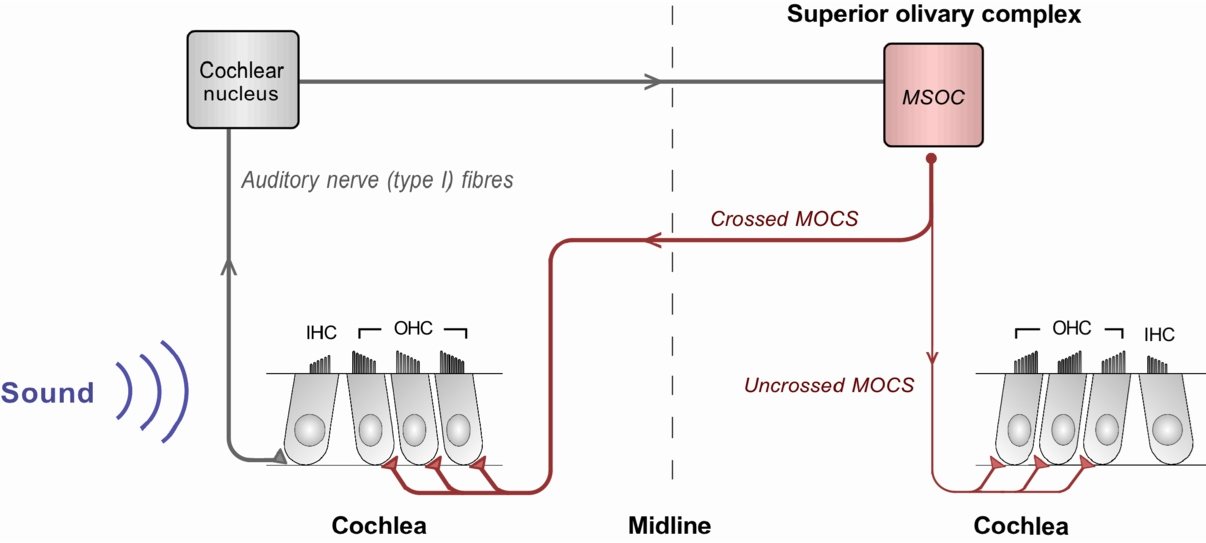
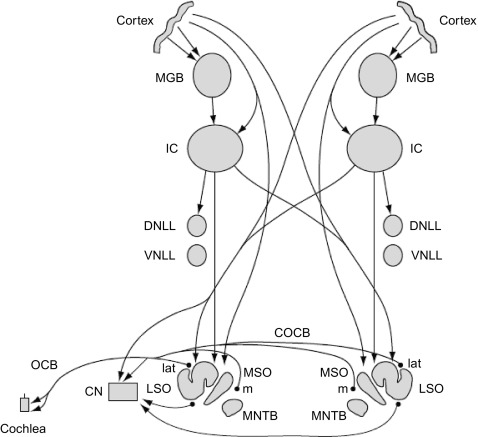
Fig: The basic MOC acoustic reflex. The auditory nerve responds to sound, sending a signal to the cochlear nucleus. Afferent nerve fibres cross the midline from the cochlear nucleus to the cell bodies of the MOCS (located near the MSOC), whose efferent fibres project back to the cochlea (red). In most mammals, the majority of the reflex is ipsilateral (shown as a thicker line), effectuated by the crossed MOCS.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3311680/
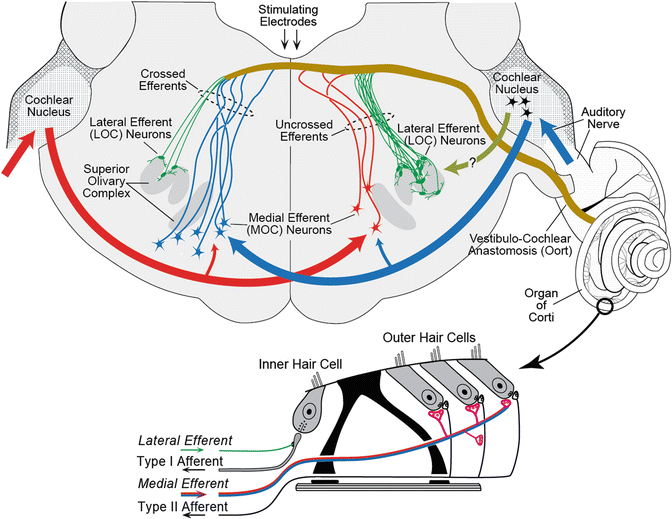
“Our ability to effectively perceive and interact with the environment integrates the activity of efferent pathways that can modulate the signals transmitted by the afferent sensory systems. In the auditory system, the efferent pathways form a neural network comprised of several feedback loops with numerous subcortical nuclei, including the thalamus, inferior colliculus, superior olivary complex, and cochlear nucleus (Malmierca and Ryugo, 2011). The auditory efferent pathways extend from auditory cortex to the peripheral sensory organ via the olivocochlear (OC) system (Figure 1). The OC system, originally described by Rasmussen (1946), is formed by two neuronal groups: (i) the medial olivocochlear neurons (MOC) and (ii) the lateral olivocochlear neurons (LOC) (Warr and Guinan, 1979).”
“ … Consequently, it has been difficult to associate deficits of olivocochlear neurons with pathogenesis, although there is some evidence of abnormal olivocochlear activity in listeners with tinnitus, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6496333/
https://pubmed.ncbi.nlm.nih.gov/2013642/
“Olivocochlear neurons have somata in the superior olivary complex and provide an efferent innervation to the cochlea. One subgroup of olivocochlear neurons, medial olivocochlear neurons, sends fibers to innervate the cochlear outer hair cells.
BvS-> After 60 years of ”normal” noise damage inner hair cells (manageable) change after an head trauma accident damage (head first into concrete pillars) into an impossible permanent ”alarm” (see more above)
Svenska (not updated)
(Nedan kan dysfunktion vara delvis ärftlig? Min mor och mormor (liksom jag) på äldre dagar hade svårt att uttrycka sig tydligt, men förmodligen på grund av deras speciella och svåra lidande kan det vara vad jag kallar dysfunktionellt ”Olivoal Cochlea (Middle Pons) – Cochlea (Outer and Inner Hair Cells) Loop” – mer arbete behövs för att undersöka detta. Bland symtomen finns kluster av hårda larmljud, där volymkontrollen i Pons troligen hade en dysfunktion – låst sig på hög ljudnivå)
Är det möjligt? Kan cochleafunktionerna (hörsel, kvantitet och kvalitet) styras från Pons med hjälp av Medial Oloviocochlar complex?
JA DETÄR MÖJLGT!
Först senaste:
Kortfattat: ”De efferenta olivokokleära (OC) är en del av hjärnstammens till hörselsnäckans reflexbanor som möjliggör stimulusrelaterad kontroll av hörselsnäckan och gör det möjligt för det centrala nervsystemet att påverka hörseln på den mest perifera neurala nivån.”
Abstract: ”Anatomin och fysiologin hos olivokokleära (OC) efferenter granskas. För att hjälpa till att tolka dessa gås också igenom de senaste framstegen inom cochleamekaniken. Laterala OC (LOC) efferenter innerverar primära hörselnervsfibrer (AN). Den viktigaste LOC-funktionen kan vara att minska auditiv neuropati. Medial OC (MOC) efferenter innerverar de yttre hårcellerna (OHC) och verkar för att minska förstärkningen av cochlean. Man har trott att cochleaförstärkning endast verkar genom basilarmembranrörelse (BM), men nya rapporter visar att rörelse nära den retikulära lamina (RL) förstärks mer än BM-rörelse, och att RL-rörelseförstärkning sträcker sig till flera oktaver under den lokala karakteristiska frekvensen. Data om efferenta effekter på AN-fiberrespons, otoakustiska emissioner (OAE) och mänsklig psykofysik granskas och omtolkas i ljuset av nya cochleamekaniska data. Det möjliga ursprunget till OAEs i RL-rörelse övervägs. Mätmetoder för MOC-effekt och MOC-inducerade förändringar i mänsklig respons granskas också, inklusive att ipsilateralt och kontralateralt ljud kan ge MOC-effekter med olika mönster över frekvenser. MOC efferenter hjälper till att minska skador på grund av akustiskt trauma. Många, men inte alla, rapporter visar att försökspersoner med starkare kontralateralt framkallade MOC-effekter har bättre förmåga att upptäcka signaler (t.ex. tal) i buller, och att MOC-effekter kan moduleras av uppmärksamhet”.
Sammanfattning: Om så är fallet får Medial Oloviocochlar (MOC) komplexet i Pons feedback från cochleaaktiviteter (funktionella eller olika grader av dysfunktionalitet) och från det kontrollåtgärder av cochlean troligen delvis via yttre hårceller och dess påverkan på inre hårcellers aktiviteter (funktionell eller olika grad av dysfunktionalitet. Om då t.ex. huvudtrauma påverkar MOC så kan ljudförvrängning relatera till detta. I mitt fall har jag 70 år av hanterbara bullerskador i samband med tinnitus som plötsligt blivit ett ohanterligt hårt permanentlarm på samma frekvens som den ”gamla, vanligare tinnitus”
En annan (tilläggande?) förklaring till min dysfunktion kan vara ”skleroserande processer” i Pons, eftersom symtomen under mina korta sömnperioder (1-2 timmar) ökar, kanske på grund av ”vävnadshårdning”: ”Perifer ponslesions plats är en bra särskiljare av MS från vaskulära lesioner.” https://pubmed.ncbi.nlm.nih.gov/32757905/
och/eller i allmänhet dysfunktioner i ”Pons: Den mellersta delen av hjärnstammen som koordinerar ansikts- och ögonrörelser, ansiktsförnimmelser, hörsel och balans.
https://my.clevelandclinic.org/health/body/21598-brainstem
Jag har haft skleroserande Basaliom Glas typ III 2017 och 2018 Prostatacancer Gleason 9 (nu väl behandlad i Helsingfors) förutom sedan 5 års MRT dokumenterad spinal dysfunktion (spondylos och foraminal spinal stenos C3-C7, L4-L5 och S1)
Arbetstext/utkast nedan
Efferenta neuroner kontrollerar hörselkänslighet och skyddar hörseln från buller genom att reglera mellanrum mellan cochleastödande celler
https://journals.physiology.org/doi/full/10.1152/jn.00468.2021
Observera ovanstående slutsats: Mediala olivokokleära efferenta nerver har innervation med cochleastödjande gap junctions och så småningom hårcellselektromotilitet, vilket kontrollerar hörselkänslighet och hörselport mot bullertrauma yttre trauma
”Det är avgörande för hörseln att det nedåtgående cochlea-efferenta systemet ger en negativ återkoppling till hårcellerna för att reglera hörselkänsligheten och skydda hörseln från buller. De mediala olivokokleära efferenta nerverna (MOC) projicerar till yttre hårceller (OHC) för att reglera OHC-elektromotiliteten, som är en aktiv cochleaförstärkare och kan öka hörselkänsligheten. Här rapporterar vi att de efferenta MOC-nerverna också kan innervera stödjeceller (SC) i närheten av OHC för att reglera hörselkänsligheten. MOC-nervfibrer är kolinerga och acetylkolin (ACh) är en primär neurotransmittor. Immunofluorescensfärgning visade att MOC-nervändar, presynaptiska vesikulära acetylkolintransportörer (VAChT) och postsynaptiska ACh-receptorer var synliga vid SC och i SC-området. Tillämpning av ACh i SC kan framkalla en typisk inåtgående ström och minska gap junctions (GJ) mellan dem, vilket följaktligen förstärkte den direkta effekten av ACh på OHC:er för att förskjuta men inte eliminera OHC-elektromotilitet. Denna indirekta, GJ-medierade hämning hade en långvarig inverkan. In vivo-experiment visade vidare att brist på denna GJ-medierade efferenta signalväg minskade regleringen av aktiv cochleaförstärkning och äventyrade skyddet mot buller. I synnerhet visade distorsionsproduktens otoakustiska emission (DPOAE) en fördröjd minskning efter exponering för buller. Våra resultat avslöjar en ny väg för det efferenta MOC-systemet via innerverande SC för att kontrollera aktiv cochleär amplifiering och hörselkänslighet. Dessa data tyder också på att denna SC GJ-medierade efferenta väg kan spela en avgörande roll i långsiktig efferent hämning och krävs för att skydda hörseln från bullertrauma.
NYTT & NOTERT Cochlear efferent system ger en negativ återkoppling för att kontrollera hårcellsaktivitet och hörselkänslighet och spelar en avgörande roll i bullerskyddet. Vi avslöjar en ny efferent kontrollväg där mediala olivokokleära efferenta fibrer har innervationer med cochleastödande celler för att kontrollera deras gap junctions, och därmed reglera yttre hårcellers elektromotilitet och hörselkänslighet. Denna stödjande cell gap junction-medierad efferent kontrollväg krävs för att skydda hörseln från buller.”
https://en.wikipedia.org/wiki/Olivocochlear_system som har efferent kontroll av och afferent återkoppling från hörselsnäckan, framför allt av yttre hårceller som ”kontrollerar” de inre, där jag har varit skadad sedan 70 år tillbaka – se audiogram (ett hypotes diagnosförslag för mitt ”5 år permanenta svårt att stå ”larm vänster sida av huvudet”, förutom 2-3 minuter under MR-undersökningen (medan höger sida hörde det typiska MR-ljudet (inte särskilt trevligt att höra) – mycket hoppfullt)”
Olivokoklearsystemet är en komponent i hörselsystemet som är involverat i den nedåtgående kontrollen av cochlean. Dess nervfibrer, olivokokleärknippet (OCB), utgör en del av den vestibulokokleära nerven (VIII:e kranialnerven, även känd som hörsel-vestibulära nerven) och skjuter ut från det övre olivarykomplexet i hjärnstammen (pons) till cochlean. https://en.wikipedia.org/wiki/Olivocochlear_system
Akustiskt framkallade svar från MOCS (medialt olivokokleärt system)
https://en.wikipedia.org/wiki/Olivocochlear_system
[Elektrisk stimulering i hjärnstammen kan resultera i (i) att hela MOCS stimuleras, (ii) en urladdningshastighet (upp till 400 s-1) som är mycket högre än vad som normalt framkallas av ljud (upp till 60 s-1), och (iii) elektrisk stimulering av andra neuroner än MOCS-fibrer. Därför kan det hända att elektrisk stimulering av MOCS inte ger en korrekt indikation på dess biologiska funktion eller den naturliga omfattningen av dess effekt.
MOC:s respons på ljud medieras genom MOC:s akustiska reflexväg (se infälld), som tidigare har undersökts med hjälp av anterograda och retrograda märkningstekniker (Aschoff et al., 1988; Robertson och Winter, 1988). Akustisk stimulering av de inre hårcellerna skickar en neural signal till den posteroventrala cochleakärnan (PVCN), och axonerna hos neuronerna från PVCN korsar hjärnstammen för att innervera de kontralaterala MOC-neuronerna. Hos de flesta däggdjur projicerar MOC-neuronerna övervägande till den kontralaterala sidan (bildar den ipsilaterala reflexen), medan resten projicerar till den ipsilaterala sidan (bildar den kontralaterala reflexen).
Styrkan på reflexen är svagast för rena toner och blir starkare när ljudets bandbredd ökar (Berlin et al., 1993), vilket innebär att den maximala MOCS-responsen observeras för bredbandsbrus (Guinan et al., 2003). Forskare har mätt effekterna av att stimulera MOCS med ljud. Hos katter visade Liberman (1989) att kontralateralt ljud (som resulterade i MOCS-stimulering) minskade N1-potentialen, en undertryckning som eliminerades vid transsektion av olivokoklearbunten (OCB). Hos människor har den största mängden bevis för efferenternas verkan kommit från undertryckandet av otoakustiska emissioner (OAE) efter akustisk stimulering.
Figur: Den grundläggande akustiska MOC-reflexen. Hörselnerven reagerar på ljud och skickar en signal till cochleans kärna. Afferenta nervfibrer korsar mittlinjen från cochleans kärna till cellkropparna i MOCS (som ligger nära MSOC), vars efferenta fibrer projicerar tillbaka till cochlean (röd). Hos de flesta däggdjur är majoriteten av reflexen ipsilateral (visas som en tjockare linje), som påverkas av den korsade MOCS.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3311680/
”Vår förmåga att effektivt uppfatta och interagera med miljön integrerar aktiviteten i efferenta vägar som kan modulera signalerna som sänds av de afferenta sensoriska systemen. I hörselsystemet bildar de efferenta vägarna ett neuralt nätverk som består av flera återkopplingsslingor med många subkortikala kärnor, inklusive thalamus, inferior colliculus, superior olivary complex och cochleakärna (Malmierca och Ryugo, 2011). De auditiva efferenta vägarna sträcker sig från hörselbarken till det perifera sinnesorganet via olivokokleära (OC) systemet (Figur 1). OC-systemet, som ursprungligen beskrevs av Rasmussen (1946), bildas av två neuronala grupper: (i) de mediala olivokokleära neuronerna (MOC) och (ii) de laterala olivokokleära neuronerna (LOC) (Warr och Guinan, 1979).
“ … Följaktligen har det varit svårt att associera underskott av olivokokleära neuroner med patogenes, även om det finns vissa tecken på onormal olivokokleär aktivitet hos lyssnare med tinnitus, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6496333/
https://pubmed.ncbi.nlm.nih.gov/2013642/
”Olivokokleära nervceller har somata i det överlägsna olivarykomplexet och ger en efferent innervation till cochlean. En undergrupp av olivokokleära nervceller, mediala olivokokleära nervceller, skickar fibrer för att innervera de yttre hårcellerna i cochlean.
BvS-> Efter 60 år av ”normala” bullerskador förändras de inre hårcellerna (hanterbara) efter en huvudtraumaolycka (huvudet före in i betongpelare) till ett omöjligt permanent ”larm” (se mer ovan)